In our family we do kind. We do hugs. We do trust. We do second chances. We do loud (really well!) We do love. We also do mental illness-with it’s accompanying therapy appointments, teacher meetings, medication, and near constant uncertainty of how to navigate a world whose opinions shouldn’t matter, but do anyway. With an alphabet soup of collected diagnosis that looks something like this…MDD-OCDGAD-SPCD-SPS-DMDD-SPDADHD-PTSD, you might be tempted to call us a hot mess. We, however, prefer the term “neurodiverse.” My particular portion of the alphabet is MDD-Major Depressive Disorder, and OCD-Obsessive Compulsive Disorder. These are not my favorite genetic gifts. The blue eyes, I was good with. The long fingers for playing the piano? Great! But those first two? They have pushed me to the brink, and threatened to send me over it more times than I can count.
What I’ve learned that I CAN count on is that I am not alone in suffering. It is part of being human. No one gets to escape, and there is no “get out of suffering free card.” (Trust me, I’ve looked!) I learn of the suffering of others each day in news articles, and in the confidences shared by friends and family. You see it in memes and printable quotes. How often have we heard to “be kind; because everyone you meet is fighting a hard battle?” We all experience it.
My own experience has taught me that as a society we split suffering into two camps: physical and mental. Physical suffering is generally accepted as something that happens to you, and is not in your control. Mental and emotional suffering are considered things that are you, and that you somehow choose or have control of. We see evidence of this in the way we speak of different conditions. We might say someone has cancer or diabetes, or a broken leg. But in our dialogue about mental and emotional well-being we say someone is mad, or sad, or, with mental illness, the person is depressed, schizophrenic, or OCD, etc.
The reality (at least my version of it) is that our brain is part of our physical body. It is subject to disease, overuse, stress, diet, thought patterns, etc. It has the power to create emotions, which our mind is left to interpret, thus creating our perceptions of the world around us. In the case of mental illness it can even produce false information and emotions that can quickly create great distress and confusion. You don’t have to have experience with mental illness to understand this. Simply think of the last dream or nightmare you experienced. The reality was that your body was safely tucked into bed. Your brain created an alternate reality of images, thoughts, sounds, and emotions that felt all too real until you were able to wake and reassess your reality.
Currently we live in a culture that is uncomfortable with the idea that mental and emotional distress even exist. It can be frightening to acknowledge that the brain can “break” with the further implication that our will, feelings, and thoughts can go rogue and not remain within our control. So discussions don’t happen. We pretend that we are immune by hiding emotions and always responding “good!” when asked how we are. The expression of challenging feelings are relegated to the therapist office, and sufferers are left to go it alone at all other times. The emphasis on getting through your challenges yourself can be seen in the number of self-care articles available online and in magazines and the sheer number of “self-help” books available on Amazon.com (70,000!)
70,000 self-help books. And still, according to the CDC, 44,193 Americans committed suicide in 2017.
Clearly our DIY approach to mental and emotional suffering is insufficient. While good and important, self-care is not always enough. I’ve considered this throughout the past year as I’ve fought to regain a sense of well-being after a relapse of depression and OCD left me struggling to accomplish even the most basic of daily tasks. My challenge was that I needed support, but felt unable to express the severity of what I was experiencing, was unsure who I could trust with this information, and had difficulty verbalizing my needs so that others could help. Likewise, because family and friends could not visibly see the level of distress I was experiencing, they did not know when or what help was needed.
I created the following framework to help bridge that gap. I’m hoping that it can be a useful tool for others to use to monitor the wellbeing of themselves and loved ones, and to especially create awareness when challenging times do arise-whether from illness, distress, or life itself.
1. Talk with a handful of family and friends that you would want to give support to, and would feel comfortable receiving support from. Create a group text or some other form of contacting one another. Consider using a simple code or scale to share how each person is doing. I’ve been using a 1-10 scale based off of this one found at https://thegracefulpatient.wordpress.com/2017/12/15/a-simple-mental-health-painscale/ You could text only when significant challenges arise, or, preferably, you could do a daily or weekly check-in with one another which would allow you to recognize when someone may be in need of support, before they reach a level of crisis.
2. If the individual shares that their distress is related to a specific condition, spend 20 minutes on Google learning about the condition, and how to provide specific support for the person who is experiencing it. Just type in “how to support someone who…” This could be anything from a clinical diagnosis to any other life stressors such as a lost job, death, big exam, move, new baby, child with a disability, loneliness, etc. www.themighty.com and www.understood.com are both great resources for understanding 100’s of different experiences.
3. When someone is in need of support, consider providing help if you are in a position to do so. Begin by insuring that the individual is safe, taking any medications needed, and seeing the proper professionals for treatment (if required.) To determine what additional support would be appreciated, simply ask “what’s hard?” Once you know what’s hard, you can assess what you can do to alleviate some of the burden.
4. Provide validation and empathy of your loved one’s experience. Here is a great short animation from Brene Brown on the difference between empathy and sympathy. https://www.bing.com/videos/search?q=Brene+Brown+Empathy+Animation&&view=d aetail&mid=40548622B1834D85D1D440548622B1834D85D1D4&&FORM=VRDGAR
5. Sometimes support is needed for a day. Other times, as with chronic conditions, it may be needed for longer periods of time. Check in as often as necessary to gauge where your loved one is at, and the level of care they might need. Continue checking in until they can give you an “all clear.”
6. Be aware of your own needs, you cannot give more than you have. Set boundaries on what you can do, and know that any level of support, acknowledgement, and empathy contributes to the well-being of your loved one.
Throughout my own journey of recovery, I have become interested in Kintsugi–the Japanese art of mending broken pottery using lacquer resin laced with gold or silver. The art provides the symbolic imagery of a philosophy that treats breaks and repairs not as signs of destruction, but as a beautiful history of the object. As we go through life, let us care for and support one another, fill in the cracks when needed, and allow there to be beauty in our collected imperfection.

When is it time to see a therapist?
How often do you consider scheduling an appointment with a therapist only to talk yourself out of getting help? It can be hard to pinpoint the...

Can I say too much to my therapist?
I was talking to an acquaintance the other day and she asked me if there was anything that should not be discussed with a therapist. I chuckled to...
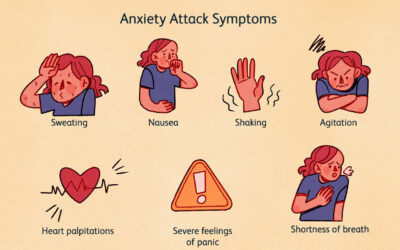
Identifying Symptoms of Anxiety
Lately, anxiety has been a major focus in the field of mental health. The media is highlighting increased levels of anxiety in our children and in...